
Sacroiliac Joint Dysfunction
- Home
- Conditions
- Back & Spine Conditions
- Sacroiliac Joint Dysfunction
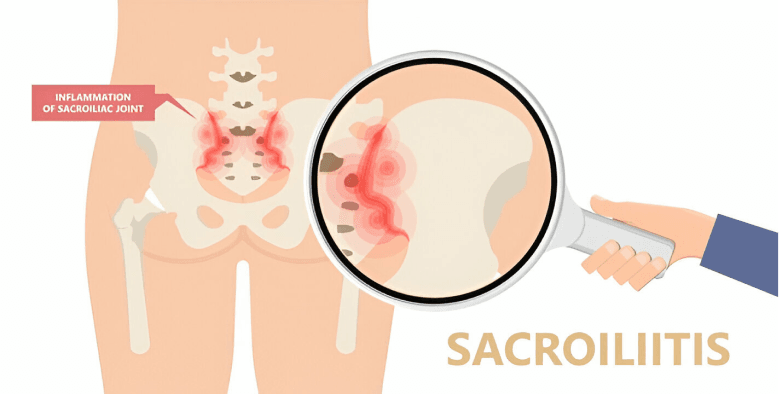
There are many different terms for sacroiliac joint problems, including SI joint dysfunction, sacroiliac joint disease, SI joint syndrome, SI joint strain, and SI joint inflammation. Each of these terms refers to a condition that causes pain in the SI joints from a specific cause.
As with most other joints in the body, the SI joints have a cartilage layer covering the bone. The cartilage allows for some movement and acts as a shock absorber between the bones. When this cartilage is damaged or worn away, the bones begin to rub on each other, and degenerative arthritis (osteoarthritis) occurs. This is the most common cause of SI joint dysfunction. Degenerative arthritis occurs commonly in the SI joints, just like other weight-bearing joints of the body.
Another common cause of SI joint dysfunction is pregnancy. During pregnancy, hormones are released in the woman’s body that allow ligaments to relax. This prepares the body for childbirth. Relaxation of the ligaments holding the SI joints together allows for increased motion in the joints and can lead to increased stresses and abnormal wear. The additional weight and walking pattern (altered gait) associated with pregnancy also places additional stress on the SI joints.
Common SI Joint Pain Symptoms
- Lower back pain (below L5)
- Sensation in lower extremity: pain, numbness, tingling, weakness
- Pelvis/buttock pain
- Hip/groin pain
- Feeling of leg instability (buckling, giving way)
- Disturbed sleep patterns due to pain
- Disturbed sitting patterns (unable to sit for long periods, sitting on one side)
- Pain going from sitting to standing
SIGNS
- Compression test
- Distraction test
- Patrick Test
- Fortwin finger test
- Thigh Thrust test
- Gaenslen test
- Gillet test
Causes of SI Joint Pain
SI joint injury is mainly caused by a combination of axial loading and rotational forces. For instance twisting while carrying a heavy object
Trauma and degeneration are the two main causes of SI joint dysfunction and pain.
What Causes SI Joint Pain?
- Sacroiliac (SI) joint dysfunction and associated pain can be caused by a specific traumatic event (disruption) or can develop over time (degeneration). Sacroiliac Trauma (common events that may cause SI joint disruption)
- Motor vehicle accident
- Fall on buttock
- Lifting and/or twisting
- Natural childbirth
- Pregnancy (chronic low back pain during and/or after pregnancy is frequently referred to pelvic girdle pain)
- Sacroiliac Joint Degeneration (common causes)
- Previous lumbar spine surgery (e.g., fusion of the lumbar vertebrae)
- Stresses to the SI joint due to leg length differences, joint replacement, or scoliosis
- Osteoarthritis
- Previous iliac crest bone graft (ICBG)
- Prior infection of the SI joint
- Ankylosing spondylitis and Rheumatoid arthritis
- Paget’s disease
- Joint infections
- Osteitis Condensans Ili
DIAGNOSIS
The diagnosis in SI joint pain is a tricky proposition as at most times no single imaging modality like x ray, CT and MRI correlate satisfactorily with the clinical picture.
MRI is generally resorted to rule out red flag signs and other disorders of the lower back.
The gold standard in diagnosis is still a LA injected into the joint and pain relief is noted.
THE IASP Criteria
- Pain present in the region of the PSIS
- Clinical tests stressing the SIJ reproducing pain
- Selectively infiltrating the putative joint with local anaesthetic complete resolves the pain
TREATMENT
Generally, these treatments can be divided into 2 categories: those directed at correcting the underlining pathology and those aimed at alleviating symptoms. To optimize outcomes, the identification and treatment of concomitant psychosocial issues is of paramount importance. This is best accomplished via a multidisciplinary approach.
Conservative Management The non-interventional management of SI joint pain should ideally address the underlining pathology. In patients with true or apparent leg length discrepancy, this might include the use of shoe inserts to more equitably distribute the load borne by the SI joints. Because leg length discrepancies are frequently found in asymptomatic individuals (37) and many patients already compensate for their lower extremity length difference by altering their gait or posture, most experts recommend starting out cautiously with inserts that correct only half the incongruity. For SI joint pain resulting from altered gait mechanics and spine malalignment, physical therapy and osteopathic or chiropractic manipulation have been reported to reduce pain and improve mobility.
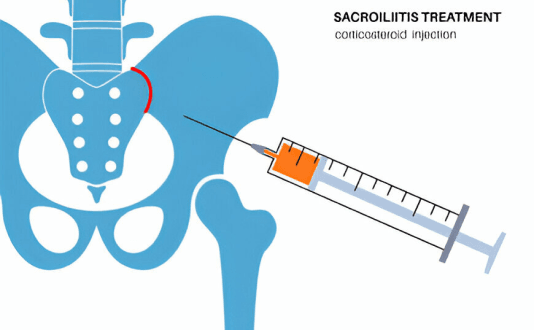
Intraarticular Injections
Intraarticular injections with steroid and LA often serve the dual function of being therapeutic and aiding in diagnosis. To summarize these studies, most but not all investigators have found radiologically guided SI joint injections to provide good to excellent pain relief lasting from 6 mo to 1 yr .
Proliferative therapy
Prolotherapy- has been advocated as a treatment for nonspecific LBP and SI joint pain The rationale behind the use of “prolotherapy” is that the ligaments and other soft tissue structures are of primary importance in the development of LBP. Thus, the injection of a drug promoting fibroblast hyperplasia should theoretically increase the strength and reduce sensitization of these structures
Radiofrequency Denervation Procedures
Several investigators have performed radiofrequency (RF) denervation procedures in an attempt to provide prolonged pain relief to patients suffering SI joint pain. The techniques used have ranged from denervating the nerves supplying the SI joint ) to creating lesions in the joint itself , with one study using a combination of the two. The success rates of studies targeting the nerve supply are higher than those focusing on the joint itself, with approximately two thirds of patients reporting significant pain relief.
Surgery
Fusion surgery is considered when all conservative measures fail
PREVENTION
- Pelvic floor exercises/ Kiegel’s exercises after pregnancy
- Avoid becoming overweight
- Some form of physical exercise to mobilises and strengthen spine
- Improved understanding of this highly misdiagnosed condition by doctors
Treatment for Sacroiliac Joint Dysfunction
Video Spotlight
Blog
Surgery-Free Solutions
Expert Tips for Pain Management



Testimonials
Words From Our Patients
The treatment was very good and the doctor Faraz Ahmed was very kind to the patient and explained clearly the procedure of knee bilateral ha & botox And we were advised to do physiotherapy. We are very much satisfied. We would recommend this alleviate pain clinic.Thank you
Got treatment of Botox and HA for right knee arthritis a month ago and finding good relief from pain. Was treated by Dr Swagtesh Bastia who explained very well about the injections and the treatment was painless. The front desk staff were very kind and very helpful and physiotherapy was also done expertly, overall good experience
Alleviate Pain Management clinic has been a godsend for my mom's knee pain. She has been treated by Dr. Wiquar Ahmed. The attentive staff provided personalised care, and after her treatment, she's feeling remarkably better. Thank you for giving my mom the relief she deserves!
The clinic is super clean with a great OT and most importantly all the staff here are very helpful and considerate. My gratitude to Dr Roshan, the nurses, and support staff - they were always available to assist with any issues post procedure and they even made an extra effort to make a home visit for a follow up check-up. This team here is the perfect example of healing and care with a human touch. Thank you!!!!!
My wife had knee pain I have visited alleviate pain and consulted doc santhoshi now she is able to walk pain free and can do her daily activity than before.the physiotherapist here Dr akhila also helped her with few exercises and the staff here Abdul explained all the procedures well . Thank you PPL can visit here for pain relief
