

Achilles Tendonitis
- Home
- Conditions
- Foot & Ankle Pain
- Achilles Tendonitis
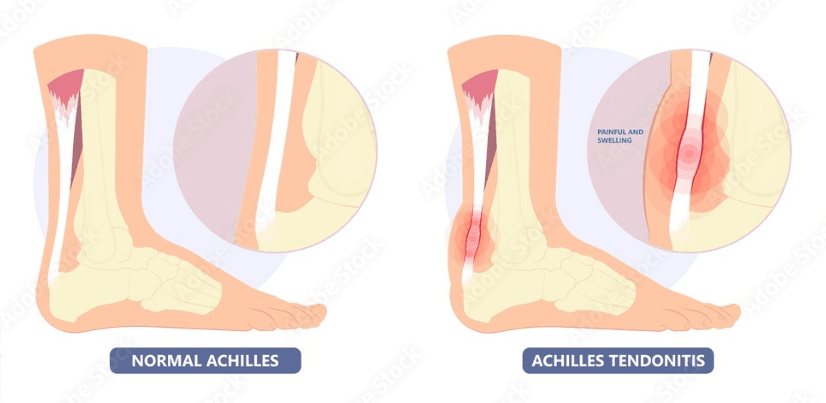
Achilles Tendonitis refers to constant irritation and inflammation of the Achilles tendon, which is the largest tendon in the body and can be found running down the back of the lower leg. Originating from the calf muscles and inserting onto the heel, the Achilles tendon can withstand great stresses while climbing, walking, running or standing up on your toes. As it experiences significant forces, the tendon stands prone to overuse and degeneration characteristic of achilles tendonitis. Patients experience the pain at the insertion of the achilles tendon onto the heel or along the substance of the tendon.
Treatment for Achilles Tendonitis
Types
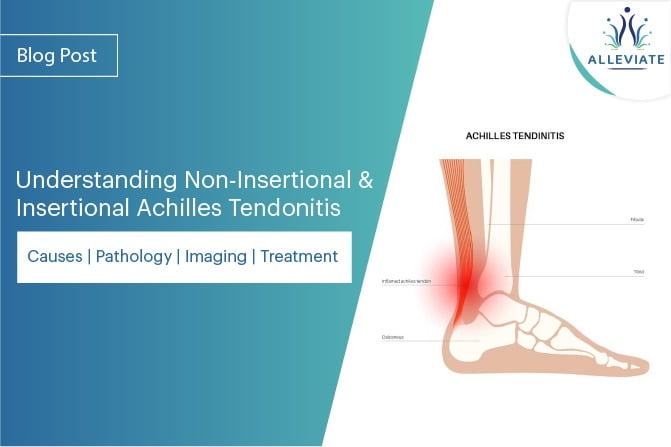
Depending on the site of the tendon inflamed, Achilles Tendonitis can be classified into Insertional and Non Insertional tendonitis.
- Non Insertional Achilles Tendinitis - Non Insertional Achilles Tendinitis Commonly seen in younger active individuals, the pathology is centred around the middle portion of the tendon exhibiting swelling, degeneration and tiny tears suggesting breakdown of the tendon fibres.
- Insertional Achilles Tendinitis - Insertional Achilles Tendonitis involves the attachment site of the tendon onto the heel bone. This is usually seen in older age groups resulting from years of overuse. Chronic cases of Insertional tendonitis are often associated with calcifications at the insertion.
Causes
This condition usually results from repetitive stress on the Achilles tendon. Some common causes observed are :
- A sudden increase in the intensity of exercise without letting the body getting a chance to acclimatize to the increased workload. Sudden drastic increase in the distance one runs daily
- Tightness in the calf muscles—Having tight calf muscles and suddenly starting an aggressive exercise program can put extra stress on the Achilles tendon
- Bone spur due to extra bone growth where the Achilles tendon attaches to the heel bone can irritate the tendon and cause pain.
- A bone spur that has developed where the tendon attaches to the heel bone.
Histopathology
The hallmark features of the tendon histopathology that are observed are cellular activation and increase in cell numbers, increase in ground substance, collagen disarray and neovascularisation. It is not considered to be a primarily inflammatory condition. Histological evaluation of biopsies shows intratendinous microdialysis, Neurogenic inflammation, though has been distinctly associated with this condition Peptides released from peptidergic group IV fibres in response to peripheral noxious stimuli are responsible for the initiation of many pathophysiological processes. Moreover, neuropeptides such as substance P and calcitonin gene- related peptide point towards an inflammatory process in the tendon.
Symptoms
The usual symptoms of Achilles tendonitis include:
- Pain and stiffness along the Achilles tendon in the morning
- Pain along the tendon or back of the heel that worsens with activity
- Severe pain the day after exercising
- Swelling that is present all the time and gets worse throughout the day with activity
A sudden pop at the back of the ankle might indicate partial or complete rupture of the Achilles tendon.
Clinical Examination
- Swelling along the Achilles tendon or at the back of your heel
- Enlargement or thickening of the Achilles tendon
- Bony spurs at the lower part of the tendon at the back of your heel indicate insertional tendonitis
- The point of maximum tenderness
- Pain in the middle of the tendon point towards no insertional tendonitis.
- Pain at the back of your heel at the lower part of the tendon is common in insertion tendonitis
- Limited range of motion in your ankle—specifically, a decreased ability to flex your foot
Investigations
X- rays can provide information on any calcification at the insertion pointing towards Insertional Achilles Tendonitis. Sometimes in cases of chronic insertional tendonitis calcifications might be noticed along the middle portion of the tendon. Additionally x rays can show additional heel spurs. MRI, though is not useful directly in the diagnosis, it is often used by surgeons for planning surgery for the diseased tendon.
Treatment
Initial Conservative Approach
Rest : The first step is to reduce the strain on the tendon by eliminating or substituting high impact activities with low impact ones. Instead of running patients are advised to use elliptical cross trainers and static cycles. In very acute and painful cases no exertion is advised till the pain comes down.
Ice : Icing the Achilles tendon a few times a day for 10-15 minute periods can help get the pain and inflammation down. Non-steroidal anti-inflammatory medications such as ibuprofen and naproxen help in managing the pain and swelling but are usually not advised for more than a week at a stretch.
Exercise and Physical Therapy : The following exercise can help to strengthen the calf muscles and reduce stress on the Achilles tendon.
Calf stretch : Calf stretch keeping the back leg straight with the heel placed on the ground one should lean forward against a wall. The front leg has a bend in the knee. To stretch the gastrocnemius complex (calf muscles) and the Achilles tendon, hips have to be pushed towards the wall in a controlled manner. Position is to be held for 10 seconds before relaxing. Exercise should be repeated around 20 times for each foot and this should give the adequate stretch in the calf muscles.
Eccentric Strengthening Protocol : Eccentric strengthening is defined as contraction of a muscle while it is getting longer. Eccentric strengthening is more helpful for non insertional tendonitis. Once initiated for a a couple of weeks under the supervision of a physical therapist, these exercises can be performed at home following that.
Heel drop : Bilateral heel drop Stand at the edge of a stair, or a raised platform that is stable, with just the front half of your foot on the stair, heels are lifted o the ground and brought back down to the lowest point possible in a controlled manner. This is to be repeated at least 20 times. Care is to be taken during the bilateral heel drop to be balanced correctly before starting.
Single leg heel drop : This exercise is similar to the bilateral heel drop, except that all the weight is balanced on one leg. Amongst other physical therapy modalities, Extracorporeal shockwave therapy(ESWT) has found some success. It produces high- energy shock wave impulses stimulating healing in the damaged tendon. Supportive Shoes and Orthotics that can o load the tendon or cushion the heel can be helpful.
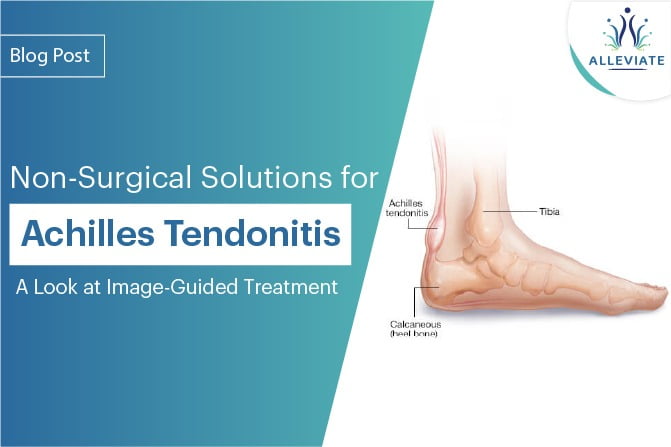
Interventional Non Invasive Approach
Blind or Ultrasound guided Cortisone injections have been used to ease the pain utilising the potent anti-inflammatory e act of cortisone. Inadvertent repeated injections of cortisone at the insertion site can cause weakening and rupture of the tendon.
Regenerative Approach
AT ALLEVIATE, we use a comprehensive approach of Platelet Rich Plasma with prolotherapy to treat Achilles Tendonitis not responding to conservative means. Procedures are carried out under strict image guidance using a high definition Musculoskeletal Ultrasound. While Prp is focussed on the insertion of the Achilles and the adjoining area of the tendon, the rest of the substance of the tendon and other adjacent calcaneal and malleolar attachments are subjected to comprehensive prolotherapy. We have seen excellent results with this treatment modality and believe should be a first line treatment o ered to patients not responding top conservative means.
Surgery
Chronic cases not responding to non-surgical means for more than 8-12 months are advised surgery. Surgeries for chronic Achilles tendonitis Gastrocnemius recession with or without debridement( usually for cases with less than 50″% of the tendon involved) Debridement with repair also augmenting it with a tendon transfer if needed is carried out usually when more than 50% of the tendon is involved. Depends upon the amount of damage to the tendon. Rehabilitation is usually started with an Air cast walking boot following the procedure.
FAQs - Achilles Tendonitis
Achilles tendonitis is a painful inflammation of the Achilles tendon, the thickest and strongest tendon in the body.
Achilles tendon is a cordlike tendon that originates from the calf muscles that runs along the back of the lower leg to the heel bone.
Achilles tendonitis is an overuse injury that causes pain and stiffness in the back of the ankle and lower leg. A patient can experience pain at the insertion of the Achilles tendon onto the heel or along with the substance of the tendon.
Based on which part of the tendon is inflamed, Achilles tendonitis has two types:
- Insertional tendonitis
- Non-Insertional tendonitis
Insertional Achilles tendonitis is Achilles tendonitis where the injury is caused by a strain or stress in the tendon where it inserts into the back of the heel bone.
Insertional Achilles tendonitis might cause is due to repeated movement or overuse stress on the Achilles tendon. The other causes might include as follows:
- Injury
- Inflammatory diseases
- Repetitive stress
- Mechanical stress
- Bony growths
- Articular disorders
- Congenital anomaly
- Tightness in the calf muscles
- Activities of daily living
- Normal aging
- Rheumatoid arthritis
- Bone spur due to extra bone growth
The signs and symptoms of Achilles tendonitis include:
- Pain - This is the most common symptom of Achilles tendonitis. The pain may be experienced as a dull, achy pain or sharp, shooting pain.
- Swelling - The area may swell because of the inflammation.
- Tenderness - You may feel tenderness when you press on the area.
- Instability - You may feel instability if Achilles tendon starts to rupture.
- Weakness - You may experience weakness if there is an injury or if you overuse the Achilles tendon.
The clinical examination of the Achilles tendon is conducted by a doctor to determine the level of injury, pain and weakness of the Achilles tendon. Your doctor will also check the maximum tenderness, and instability.
Ultrasonography is the primary imaging test for the Achilles tendon. It helps to reveal any structural abnormalities like tears, tendinopathy, swelling, calcifications and bursitis. X-rays help in determining Insertional Achilles Tendonitis. MRI or CT scans are done in case of suspected tendon rupture.
The treatment for an Achilles tendon typically includes:
- Rest
- Ice
- Non-steroidal anti-inflammatory medications
- Exercise and Physical Therapy
Rest is the initial step to reduce the strain on the Achilles tendon by eliminating or substituting high-impact activities with low-impact ones. Patients are advised to use elliptical cross trainers and static cycles instead of running. In some the cases like acute and painful cases, the high exertion should be limited.
After an Achilles tendon rupture, icing will help decrease swelling and inflammation. Apply an ice pack to the injured area for about 15 to 20 minutes a day for few times. Do not apply ice if you have an open wound.
Yes. Non-steroidal anti-inflammatory medications (NSAIDs) such as ibuprofen and naproxen help in managing mild to moderate pain and swelling. Usually, NSAIDs are not prescribed for more than a week at a stretch.
The exercise and physical therapies can help in strengthening the muscles and reduce stress on the Achilles tendon.
Finding the right exercises and physical therapy may be used to help to treat Achilles tendonitis. Some of the types included are:
- Calf stretch
- Eccentric Strengthening Protocol
- Heel drop
Surgery is the last resort if non-surgical methods do responsive for more than 8-12 months. Surgery is performed for chronic Achilles tendonitis. Depending on the damage of the tendon, the Gastrocnemius recession or Debridement method is conducted.
Rehabilitation usually begins with an Air cast walking boot post-procedure.
The Alleviate Pain Clinic offers holistic treatment approach for those suffering from Achilles tendonitis. We have a clinic a short distance from your home. Call us today at 080 2361 4888 OR +91 9620244761.
Video Spotlight
Blog
Surgery-Free Solutions
Expert Tips for Pain Management

Testimonials
Words From Our Patients
The treatment was very good and the doctor Faraz Ahmed was very kind to the patient and explained clearly the procedure of knee bilateral ha & botox And we were advised to do physiotherapy. We are very much satisfied. We would recommend this alleviate pain clinic.Thank you
Got treatment of Botox and HA for right knee arthritis a month ago and finding good relief from pain. Was treated by Dr Swagtesh Bastia who explained very well about the injections and the treatment was painless. The front desk staff were very kind and very helpful and physiotherapy was also done expertly, overall good experience
Alleviate Pain Management clinic has been a godsend for my mom's knee pain. She has been treated by Dr. Wiquar Ahmed. The attentive staff provided personalised care, and after her treatment, she's feeling remarkably better. Thank you for giving my mom the relief she deserves!
The clinic is super clean with a great OT and most importantly all the staff here are very helpful and considerate. My gratitude to Dr Roshan, the nurses, and support staff - they were always available to assist with any issues post procedure and they even made an extra effort to make a home visit for a follow up check-up. This team here is the perfect example of healing and care with a human touch. Thank you!!!!!
My wife had knee pain I have visited alleviate pain and consulted doc santhoshi now she is able to walk pain free and can do her daily activity than before.the physiotherapist here Dr akhila also helped her with few exercises and the staff here Abdul explained all the procedures well . Thank you PPL can visit here for pain relief
