

Quadriceps Tendonitis
- Home
- Conditions
- Knee pain
- Quadriceps Tendonitis
The knee being one of the major weight bearing joint in our body, absorbs a lot of stress over the years. Years of stresses across the joint can lead to overuse and malalignment in the structures of the knee joint. This further leads to strain, irritation and inflammation of the quadriceps tendon and can sometimes even lead to tears in the tendon. This may manifest as nagging pain above the knee which maybe associated with swelling and weakness in the functioning of the quadriceps. Quadriceps tendonitis is essentially an overuse injury and sports which are the usual culprits are running, football and volleyball.
Treatment for Quadriceps Tendonitis
Relevant Anatomy
The quadriceps mechanism involves the confluence of the large quadriceps muscle into a tendon. The patella is cushioned inside the tendon, and this tendon further extends inferiorly from the patella and goes and inserts into the tibial tubercle on the tibia. The tendon along with the patella essentially comprise the quadriceps mechanism. Though functionally the tendon is treated as one, it comprises of two different structures, the quadriceps tendon inserting on the upper half of the patella and the patellar tendon which is the continuity of the tendon from the lower end of the patella inserting onto the tibial tubercle.
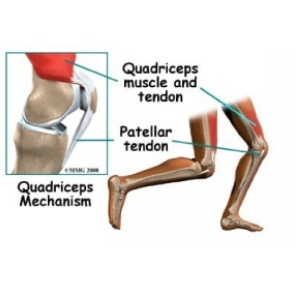
Contraction of the quadriceps brings about straightening of the knee. The patella acts as a fulcrum whereas the Femur (thigh bone) and Tibia (leg bone) act as levers subjecting the knee joint and surrounding structures to massive loads. The joint reaction forces are two to three times body weight during walking and upto five times while running.
Causes
- An overuse injury, the cause for Quadriceps tendonitis might be intrinsic or extrinsic.
- Extrinsic – These factors which include improper footwear, errors in training protocols and very importantly regular playing and training on hard unforgiving surfaces like cement. Generally excessive training(duration and intensity) and rapid escalation in level of training can be major risk factors for developing quadriceps tendonitis.
- Intrinsic – These are host specific factors and include age, flexibility, and joint laxity. Some of the specific host characteristics which predispose an individual are
- Malalignment of the foot, ankle, and leg
- Flat foot (pes planus)
- Patellar maltracking
- Rotation of tibia
- Leg length discrepancy
- Obesity
- Pathology – The strength of the quadriceps tendon is directly proportional the size, number and orientation of the constituent collagen fibres. A mismatch between the load on the quadriceps and it’s ability to satisfactorily distribute the force can lead to Overuse. This mismatch or overuse can weaken the tendon over time and make it ripe for an impending injury. Repeated microtrauma at the muscle tendon junction can prevent full healing. Tissue breakdown can lead to inflammation and tendonitis ensues (can also cause partial tears). Chronic tendonitis eventually leads to a condition called Tendinosis.
Symptoms
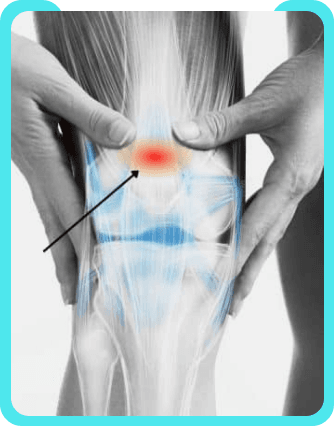
- Patients typically localise the pain to the bottom of the thigh, just above the knee cap. Movements of the knee joint can aggravate the pain in this area of tendon attachment.
- Sometimes the presentation might include a swelling in the distal thigh, Swelling might be very tender to touch in some cases. Stiffness is usually described in the mornings just after waking up(following a period of relative immobilisation) or after exercise.
Diagnosis
Clinical examination is carried out after through history taking. Tenderness can be usually elicited with palpation of the quadriceps tendon insertion. The knee is examined for range of movement, detecting laxity and structural integrity in various planes. The clinician should rule out intrinsic and extrinsic factors affecting the knee eg. sudden changes in training habits. Alignment of the knee, foot and ankle is checked. In case of a ruptured quadriceps tendon, a gap might be palpated at the insertion site. Weakness in the extensor mechanism might be indicative of insufficiency of the quadriceps. An X-ray of the knee can show fractures or the presence of calcium deposits in the quadriceps muscle but these do not pick up soft tissue injuries. High definition.

Ultrasound and MRI are the preferred investigations in diagnosing tears, tendonitis and tendinitis. Ultrasound can be further helpful in guiding Regenerative treatments like Platelet Rich Plasma and Prolotherapy.
Treatment
Conservative Treatment
- The initial treatment initiated usually involves rest, ice , elevation and anti-inflammatory medication.
- The offending activity (e.g running) must be stopped. Relative rest to gradually increasing activities promoting recovery is the way to go.
- However if the patient experiences pain at rest, Immobilisation with a splint or brace is initially undertaken.
- Relative rest is a term used to describe a process of rest-to-recovery based on the severity of symptoms.
- Pain at rest means strict rest and a short time of immobilization in a splint or brace is required.
- When pain is no longer present at rest, then a gradual increase in activity is allowed so long as the resting pain doesn’t come back.
- Physical therapy plays an extremely crucial role in rehabilitation.
- Modalities like ice massage, local ultrasound application and electrical stimulation help in limiting the pain and inflammation.
- Stretching and strengthening exercises serve the purpose of correcting muscle imbalances.
- Eccentric Muscle strengthening helps in patients where the contributing factor is constant eccentric muscle loading in closed chain kinetic activities.( Closed chain- foot is in contact with the ground)Heat may be used in cases of chronic tendinosis as it helps in boosting blood circulation and promotes tissue healing.
- Bracing and taping of the patella makes exercises less painful.
Interventional Pain Management & Regenerative Medicine
Platelet Rich Plasma with Prolotherapy – In our experience, we have seen the best results in patients who undergo PRP with prolotherapy, follow a structured exercise regime and are ready to incorporate lifestyle and nutritional modifications to improve the environment of the affected tendon to heal. Image guidance in the form of a high definition ultrasound is used. PRP is delivered at the site of maximum pathology and the rest of the structures are treated with dextrose prolotherapy. Sometimes, local steroid injection to reduce the inflammation must be undertaken. Care must be taken to avoid successive steroid injections as they can weaken the muscle.
Surgical Intervention
If nonsurgical treatment fails to serve the purpose,, surgery may be suggested. Surgery is aimed at stimulating healing through revascularization (restoration of blood supply). Damaged tissue is removed and the tendon is repaired. A well-planned rehabilitation program lets most patients return to their previous level of activity without recurring symptoms.
FAQs - Quadriceps Tendonitis
Quadriceps tendonitis is a painful condition in the quadriceps of the muscles and tendons in the areas of knee structures. It causes inflammation due to overuse and malalignment in the structures of the knee joint. Tendonitis can also affect the knee, joints, hip, ankle, or quadriceps. Overall, quadriceps tendonitis is usually associated with an overuse injury and sports.
Quadriceps Tendonitis injuries are due to injuries from playing sports. Excessive training and rapid escalation in the duration of training are other factors that contribute to quadriceps tendonitis injuries. It also causes by wearing improper footwear might cause injuries related to tendonitis.
Running on hard surfaces is the cause of getting quadriceps tendonitis injuries.
Anyone can get quadriceps tendinitis, and athletes have a higher risk. Often, quadriceps tendinitis gets better within weeks, but sometimes it prolongs. For better results, consult the best pain management specialist for effective treatment.
The risk factors for quadriceps tendonitis include:
- Age factor
- Athletes – people who run, jump, play sports like volleyball or soccer
- Chronic diseases like diabetes
- Obesity
- Rheumatoid arthritis
- Gout
- and other chronic alignments
Patients suffering from quadriceps tendonitis will have pain at the bottom of the thigh above the patella (knee cap).
- Aggravate pain in the areas of tendons
- Swelling in the distal thigh
- Stiffness in the knee in the early morning
- Warmth or burning pain around the affected areas
Clinical examination will be carried to assess full physical examination. The knee movement of the knee is examined Discussing the routine activity and sports-related activities (if any) with the doctor Your physician will look for torn or ruptured tendons in the quadriceps
Tests that are carried out include:
- X-Ray – to detect fractures or the calcium deposits present in the quadriceps muscle
- Ultrasound and MRI scans to determine the tears, tendonitis, and tendinosis
Treatment options available for quadriceps tendonitis are:
- Conservative treatment
- Interventional Pain Management & Regenerative Medicine
- Surgical Intervention
Treatment for quadriceps tendonitis is purely based on patient-to-patient. Most patients are recovered through non-surgical methods. The treatment can be of a combination of multiple procedures depending on the condition and severity.
The first-line of conservative treatment usually involves:
- Rest: helps in protecting the injury, limiting movements of the knees that are overused. During the period of rest, a short time of immobilization in a splint or brace is required.
- Ice: Applying ice around the swelling or the affected area will help in minimizing pain and swelling.
- Elevation: It helps in relieving pain, raising your knee on the elevated surface will minimize the swelling.
- Anti-Inflammation: Medications help in limiting the pain, relief from pressure, and increasing stability.
Physical therapy and exercises play a crucial role during the rehabilitation process. Getting in touch with physical therapists will help you guide with the best plan of therapies.
The other modalities of treatment that helps in reducing pain are:
- Massage
- Local Ultrasound Application
- Electrical Stimulation
Stretching and strengthening exercise serves the purpose of correcting muscle imbalances. Eccentric Muscle strengthening helps in the cases of chronic tendinosis, boosts blood circulation, and promotes tissue healing.
Platelet Rich Plasma with Prolotherapy is widely known to yield the best results in patients. PRP is delivered using image guidance in the form of high-definition ultrasound. Local steroid injections are sometimes used to reduce inflammation.
Patient should strictly follow a structured exercise regime. Nutrition modifications should be incorporated into the lifestyle. Hence, your nutritionist will execute the plan.
Most patients are treated with non-surgical treatment options. In most cases, either with conservative treatment or interventional pain management treatment, a high success rate has emerged.
A surgical option is the last option if all the non-surgical techniques are failed. It aims to stimulate the healing process through revascularization (restoration of blood supply). During this procedure, damaged tissue is removed and the tendon is repaired. Post-treatment guidelines should be strictly followed for a well-planned rehabilitation program.
Video Spotlight
Blog
Surgery-Free Solutions
Expert Tips for Pain Management



Testimonials
Words From Our Patients
The treatment was very good and the doctor Faraz Ahmed was very kind to the patient and explained clearly the procedure of knee bilateral ha & treatment And we were advised to do physiotherapy. We are very much satisfied. We would recommend this alleviate pain clinic.Thank you
Got treatment of Treatment and HA for right knee arthritis a month ago and finding good relief from pain. Was treated by Dr Swagtesh Bastia who explained very well about the injections and the treatment was painless. The front desk staff were very kind and very helpful and physiotherapy was also done expertly, overall good experience
Alleviate Pain Management clinic has been a godsend for my mom's knee pain. She has been treated by Dr. Wiquar Ahmed. The attentive staff provided personalised care, and after her treatment, she's feeling remarkably better. Thank you for giving my mom the relief she deserves!
The clinic is super clean with a great OT and most importantly all the staff here are very helpful and considerate. My gratitude to Dr Roshan, the nurses, and support staff - they were always available to assist with any issues post procedure and they even made an extra effort to make a home visit for a follow up check-up. This team here is the perfect example of healing and care with a human touch. Thank you!!!!!
My wife had knee pain I have visited alleviate pain and consulted doc santhoshi now she is able to walk pain free and can do her daily activity than before.the physiotherapist here Dr akhila also helped her with few exercises and the staff here Abdul explained all the procedures well . Thank you PPL can visit here for pain relief
