
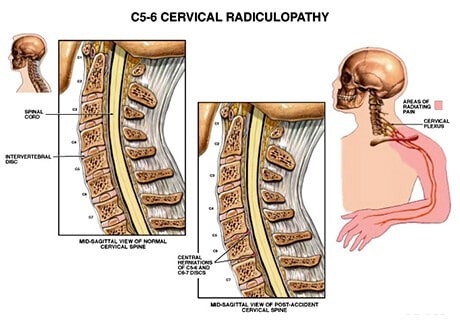
CERVICAL RADICULOPATHY
ETIOPATHOGENESIS

Degenerative Cervical disc disease- There are six jelly like cervical discs which act as natural shock absorbers present in the neck. Disc is structurally filled on the inside with a mucoprotein gel and is referred to as the nucleus pulposus. The nucleus pulposus is a thin yet flexible layer of woven cartilage strands known as the annulus fibrosus. The discs are essentially filled with water and as the age advances, the water content starts decreasing. In certain cases this dehydration of the discs is pretty rapid and this makes the annulus susceptible to cracks and tears. Due to absence of an indigenous blood supply, tears in the discs have a high chance to go unhealed or form structurally weak scar tissue which again is a potential site of tear in the future.

Traumatic Cervical Disc Migration- Road Traffic Accidents, sports injuries and falls are some of the causes of a traumatic cervical disc migration.

Cervical foraminal stenosis- Narrowing of a foramen(bony opening where a nerve root exits the spinal canal) can cause the adjacent nerve root to get pinched. Osteophytes(bone spurs) resulting due to degenerative arthritic changes in the cervical spine, a bulging disc or thickened ligaments might cause compression of the nerve root. Foraminal Stenosis is the single most common cause for cervical radiculopathy.
CLINICAL PRESENTATION
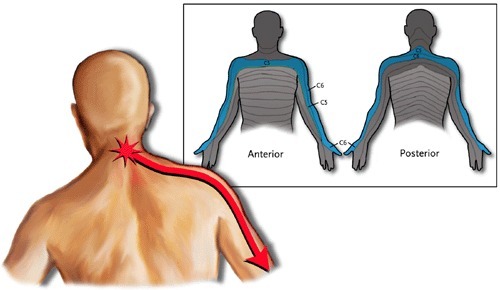
- Radiating pain due to nerve compression can be experienced which tends to be a sharp, electric shock like pain radiating down from the neck, along the shoulder Travelling further into the arm, hand and fingers.
- Neurological symptoms such as pins, needles, tingling,numbness and weakness can accompany the pain in the upper limbs. These can interfere with routine activities such as typing, holding and getting dressed.
- Pain due to the disc (discogenic pain)is usually aggravated by movements of the neck and is relieved by rest.When the pain is primarily discogenic, there is a higher chance of resolution by itself but if there is disc migration or bone spur causing a pinched nerve root and associated symptoms, it would be advisable to initiate treatment for the same.
RADICULOPATHIES AT INDIVIDUAL LEVELS
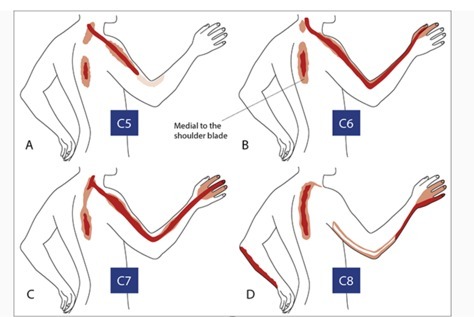
- C5 radiculopathy. This might present as pain associated with tingling and numbness which might radiate down from the neck into the shoulder and going down the arm upto the thumb. Patient might experience some weakness in the shoulder and upper arm.
- C6 radiculopathy. Radiation of symptoms usually follows the arm into the index finger. Weakness might be elicited in the biceps or the wrist.
- C7 radiculopathy. Tingling, numbness, and/or pain may be felt down the arm and into the middle finger. Weakness might be experienced in the triceps.
- C8 radiculopathy. Symptoms may radiate down the arm and into the little finger. Handgrip strength might be reduced.

DIAGNOSIS
A thorough history can be extremely informative in guiding our diagnosis towards Cervical Radiculopathy. Patients suffering with radiculopathy usually present with unilateral pain. Next comes the clinical examination including relevant sensory and motor examination which helps us in localising the level of the lesion responsible for the radiculopathy.
Distribution of sensory and motor weaknesses typically seen with cervical radiculopathy
- Level Muscle weakness Sensory deficits/location of pain ReflexC5 Deltoid Lateral arm BicepsC6 Biceps
- Wrist extension Radial forearm
- Radial two digits BrachioradialisC7 Triceps
- Wrist flexion Middle finger TricepsC8 Finger flexors ulnar two digits T1 Hand intrinsics Ulnar forearm
Popular provocative tests
Provocative tests are carried out to aid in the diagnosis of cervical radiculopathy.The aim of these tests is to bring about narrowing of the foramen which will most likely reproduce the symptoms of Cervical Radiculopathy.
These are namely
- Spurling test- This involves axial loading of the cervical spine along with rotation.(with or without extension) This test has very high specificity(94%) as compared to the other provocative tests
- Shoulder Abduction test
- Neck distraction
- Elveys upper limb tension test
AT ALLEVIATE,We go a step further and after the inflammation settles down following the steroid injection, we couple it up with successive sessions of Platelet Rich Plasma with Prolotherapy to strengthen the integrity of the cervical spine and the associated soft tissue structures. This is coupled with a structured physical therapy program and inputs from Clinical Nutrition and Clinical Psychology as and when necessary.
Differential Diagnosis
- Cervical Myelopathy- Patients present with signs such as altered gait pattern, hyperreflexia and find it difficult to accomplish fine motor tasks such as writing and buttoning shirts. These are essentially signs of Upper Motor Neuron lesions.
- Peripheral Nerve Compression- Median or Ulnar Nerve Entrapment might cause confusing overlapping symptoms. The clinician should also be mindful of a “double crush” phenomenon which involves cervical radiculopathy accompanied by a peripheral nerve entrapment.
- Shoulder pathologies can also present with similar symptoms and should ne ruled out.
- Uncommon differential diagnosis include cardiac pain, herpes zoster(shingles), Parsonage Turner syndrome, postmedian sternotomy lesion, intra and extraspinal tumors, and thoracic outlet syndrome.
Imaging
X rays of the cervical spine with AP and Lateral projections are helpful to observe the disc height and presence of degenerative changes.MRI remains the gold standard imaging modality to assess the soft tissue sources of impingement as well as any changes indicating myelopathy.CT scans give clearer idea about bony pathology and may be used to better delineate “hard” disc impingement.
Non-operative treatment
The conservative approach includes immobilisation, physical therapy , manipulation and medical management.
Immobilization- Immobilisation carried out with a soft cervical collar has been tried to limit inflammation and reduce the irritation of the nerve root but this kind of mobilisation has not received much evidential support over the years.
Physical therapy- The physical therapy modalities which are commonly used in the management of cervical radiculopathy include Intermittent Local Ultrasound and Infrared application and Stretching and strength training of the neck muscles.The intensity of the physical therapy program is started cautiously and slowly amped up. Postural and ergonomic training should also be included in the physical therapy program.
Cervical Traction- Cervical Traction has been a popular modality over the years in the past but in the last decade many clinicians have abandoned the use of traction for treating cervical pathologies because many studies reaching a consensus that traction does very little in the management of cervical radiculopathy.

Manipulation- Benefits of manipulation in treating cervical radiculopathy is definitely uncertain. Gross et al in their Cochrane review in assessing the efficacy of manipulation in managing neck pain, concluded that there were no discernible differences in the outcomes of patients treated with manipulation in the immediate,shot-term and intermediate follow up period.

Medication- NSAIDS are used in the management of cervical radiculopathy owing to their anti-inflammatory and analgesic actions. Oral steroid medications are sometimes given in the acute phase to dampen the inflammatory cascade. Narcotic medications are used in some cases but caution has to be exercised to prevent dependence.Image guided Cervical Epidural Anti-inflammatory Injection Anti-inflammatory corticosteroid injections delivered in the cervical epidural space are an excellent treatment option for a vast majority of patients. These provide relief by reduce inflammation at the nerve root, decreasing nociceptive input from somatic nerves, stabilizing effect on neural membranes and by blocking the synthesis of pain-mediating neuropeptides. Corticosteroids are also known to break up adhesions at the site of injections and block C-fibre activity in the dorsal root ganglion.
Operative treatment
Patients not responding to sincere attempt at conservative management are considered for surgical interventions. The choices of surgical interventions are as follows
- Anterior Cervical Discectomy with decompression
- Cervical Disc Arthroplasty
- Posterior decompression
FAQs - CERVICAL RADICULOPATHY
Cervical Radiculopathy is compression from the herniated disc material or associated with arthritis spurts. It typically generates neck pain or numbness that radiates from the neck to the arm, or sensory disturbances, and weakness in the muscles of the upper limbs. Wear and tear of the supporting discs are evident in the radiculopathy.
Cervical radiculopathy is often caused due to degenerative spine as age progresses or by an injury that causes a herniated disc. In young people, it can also cause injury due to accidents or sports. It can cause traumatic cervical migration. Osteophytes (bone spurs) also result due to degenerative arthritic that occurs in the cervical spine.
• degenerative Cervical disc disease
• traumatic cervical disc migration
• cervical foraminal stenosis
• degenerative Cervical disc disease
• traumatic cervical disc migration
• cervical foraminal stenosis
Yes, it is permanent only in isolated cases. One may feel numbness and/or weakness in the arms, shoulders, and hand irrespective of undergoing different treatments. If not shown at the right time or if the treatment is delayed, the condition might be permanent, or even it can lead to paralysis.
Most patients who undergo cervical radiculopathy treatment will usually get healed from 4 to 6 months of the treatment or even earlier.
Symptoms of the radiculopathy or pinched nerve are as follows:
• Radiating pain due to nerve compression – it can tend to sharpen the pain from the neck to shoulder and further to arms, hands, and fingers.
• Neurological symptoms like pin, needles, tingling, numbness, and weakness are associated with the upper limbs.
• Pain due to the disc (discogenic pain). Pain can be aggravated that affects neck movements. • Routine life is affected due to pain in the pinched nerve
• Radiating pain due to nerve compression – it can tend to sharpen the pain from the neck to shoulder and further to arms, hands, and fingers.
• Neurological symptoms like pin, needles, tingling, numbness, and weakness are associated with the upper limbs.
• Pain due to the disc (discogenic pain). Pain can be aggravated that affects neck movements. • Routine life is affected due to pain in the pinched nerve
If you come across radiating pain, neurological symptoms, or discogenic pain that affects routine activities should immediately consult with the doctor.
If not treated at the right, the condition worsens, which might even lead to paralysis.
Spurling test is the highest level of test to confirm the diagnosis of cervical radiculopathy. Cervical Myelopathy, Peripheral Nerve Compression, Shoulder Abduction test, and Elveys upper limb tension test.
Imaging tests such as X-Rays, MRI scans, and CT scans help in detecting the degenerative presence of the disc, assessing soft tissues, and getting clear visibility of the bony pathology.
Imaging tests such as X-Rays, MRI scans, and CT scans help in detecting the degenerative presence of the disc, assessing soft tissues, and getting clear visibility of the bony pathology.
Both non-operative and operative treatment methods are available to treat cervical radiculopathy. Patients not responding to non-operative methods are treated with the operative procedures. However, most of the positive results are from non-surgical procedures.
Immobilization, Physical therapy, Manipulation, and Medication are non-operative treatments available to resolve pinched nerve problems.
Immobilisation method involves minimizing the inflammation and reducing the irritation of the nerve root is performed.
Physical therapy for cervical radiculopathy cautiously involves limiting down the pain and increasing mobility.
Therapies involve are Intermittent Cervical Traction, Local Ultrasound, and Infrared application.
Stretching and strength training of the neck muscles helps in improvising flexibility and posture.
Postural and ergonomic training the certified physical therapists are also included.
Therapies involve are Intermittent Cervical Traction, Local Ultrasound, and Infrared application.
Stretching and strength training of the neck muscles helps in improvising flexibility and posture.
Postural and ergonomic training the certified physical therapists are also included.
The main aim of using the manipulation procedure is to improvise mobility, manage the neck pain, and increase the better healing process.
NSAIDS are used in managing cervical radiculopathy that brings down inflammation and irritation. Oral steroids have sometimes been used that act as anti-inflammation drugs. Narcotic medications are sometimes used but under prescription.
Image-guided Cervical Epidural and Corticosteroid injections are the Anti-inflammatory Injections in cervical epidural space. It helps in reducing inflammation at the nerve root, minimizing nociceptive input from the nerves, and stabilizing the membranes.
Anterior Cervical Discectomy with decompression, Cervical Disc Arthroplasty, and Posterior decompression are the surgical treatments to treat cervical radiculopathy.
Doctors who have successfully treated patients through a non-surgical process are the best option. Most of the cases yield results through non-operative procedures by highly experienced pain management specialists.
Testimonials
References
[1]. Rhee JM, Yoon T, Riew KD. Cervical radiculopathy. J Am Acad Orthop Surg. 2007;15:486–94. doi: 10.5435/00124635-200708000-00005. [PubMed] [CrossRef] [Google Scholar]
[2]. Wainner RS, Gill H. Diagnosis and nonoperative management of cervical radiculopathy. J Orthop Sports Phys Ther. 2000;30:728–44. doi: 10.2519/jospt.2000.30.12.728. [PubMed] [CrossRef] [Google Scholar]
[3]. Rubinstein SM, Pool JJ, van Tulder MW, et al. A systematic review of the diagnostic accuracy of provocative tests of the neck for diagnosing cervical radiculopathy. Eur Spine J. 2007;16:307–19. doi: 10.1007/s00586-006-0225-6. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
[4]. Eubanks JD. Cervical radiculopathy: nonoperative management of neck pain and radicular symptoms. Am Fam Physician. 2010;81:33–40. [PubMed] [Google Scholar]
[5]. Caridi JM, Pumberger M, Hughes AP. Cervical radiculopathy: a review. HSS J. 2011;7:265–72. doi: 10.1007/s11420-011-9218-z. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
[6]. Dreyer SJ, Boden SD. Nonoperative treatment of neck and arm pain. Spine (Phila Pa 1976) 1998;23:2746–54. doi: 10.1097/00007632-199812150-00016. [PubMed] [CrossRef] [Google Scholar]
[7]. Cheng CH, Tsai LC, Chung HC, et al. Exercise training for non-operative and post-operative patient with cervical radiculopathy: a literature review. J Phys Ther Sci. 2015;27:3011–8. doi: 10.1589/jpts.27.3011. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
[8]. Diab AA, Moustafa IM. The efficacy of forward head correction on nerve root function and pain in cervical spondylotic radiculopathy: a randomized trial. Clin Rehabil. 2012;26:351–61. doi: 10.1177/0269215511419536. [PubMed] [CrossRef] [Google Scholar]
[9].Gross A, Langevin P, Burnie SJ, et al. Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. Cochrane Database Syst Rev. 2015;9 [PubMed] [Google Scholar]
© 2020-21 Alleviatepainclinic. All rights reserved.