

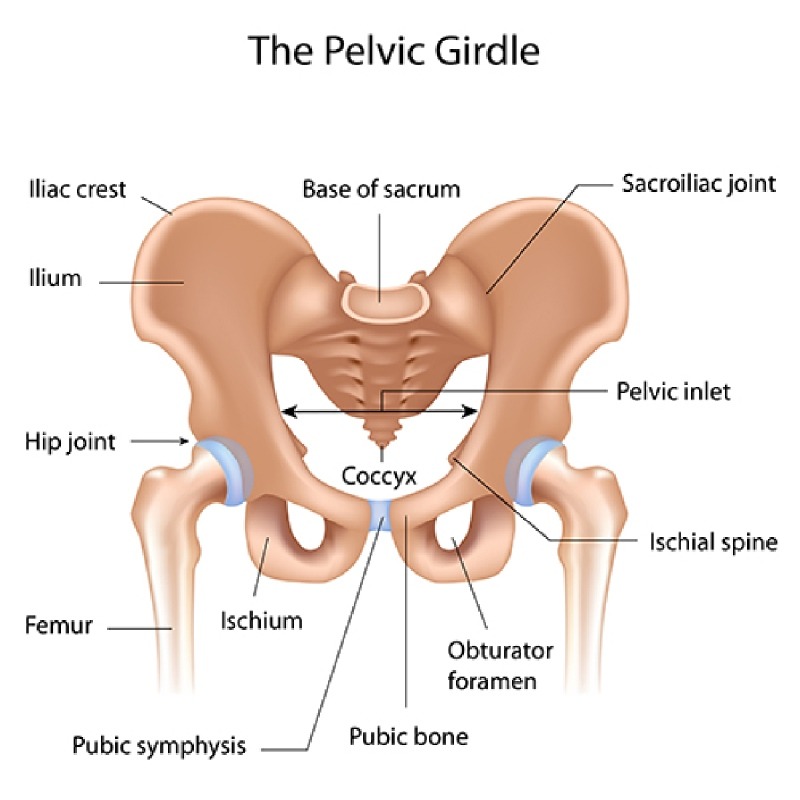
ANATOMY OF THE COCCYX
Coccyx is the distal most part of the spine. It is triangular in shape and comprises of 3-5 fused segments. It serves as one leg of the tripod, also comprising of the two ischial tuberosities and this tripod forms the weight bearing surface in a seated position. It forms a central connecting point for various pelvic floor muscles which support the anus, vagina in females and also play a supporting role in defecation, walking and running. (Diagram to be added)
PREVALANCE & ETIOLOGY
Coccydynia has shown a preponderance towards women and
overweight individuals. It shows a prominent gender bias with women affected five times more than men. Moreover,
adolescents and adults are more commonly predisposed to developing Coccydynia as
opposed to the prepubertal age group
 External Trauma – This can result due to fall backwards leading to bruising, dislocation or a fracture of the coccyx. Prolonged sitting on surfaces that are hard, not wide enough and lead to an uncomfortable posture can result in Coccydynia.
External Trauma – This can result due to fall backwards leading to bruising, dislocation or a fracture of the coccyx. Prolonged sitting on surfaces that are hard, not wide enough and lead to an uncomfortable posture can result in Coccydynia.
 Internal Trauma – Sometimes prolonged or obstructed labour, especially ones necessitating instrumentation can predispose the coccyx to injury owing to its proximity to the birth passage.
Internal Trauma – Sometimes prolonged or obstructed labour, especially ones necessitating instrumentation can predispose the coccyx to injury owing to its proximity to the birth passage.
 Degenerative disc disease
Degenerative disc disease
 Anatomical variants of the coccyx
Anatomical variants of the coccyx
 Increased or decreased laxity of the sacrococcygeal joint
Increased or decreased laxity of the sacrococcygeal joint
 Infectious origin, eg Tuberculosis of the Coccyx
Infectious origin, eg Tuberculosis of the Coccyx
 Tumors(rare)
Tumors(rare)
 Somatization and psychological can also be associated at times with tail bone pain
Somatization and psychological can also be associated at times with tail bone pain
Alternate terminology for Coccydynia used frequently
Symptoms

Pain is generally localised to the tail bone area without radiation into the gluteal region and lower extremities. Patients usually complain of a dull, achy soreness which can vary in intensity. The intensity of the pain and discomfort fluctuates with changes in posture and pressure.

The neurotransmitters Substance P and glutamate are found in increased levels in patients suffering with Fibromyalgia. These constitute the targets of pregabalin and gabapentin, which help in promoting sleep, alleviating anxiety and modulate pain.

Getting up from a sitting position might be painful and in some cases the person may need to lean for support while standing or sitting.

Close proximity to the rectum and genitalia can lead to worsening of pain during intercourse and defecation.

DIAGNOSIS
Careful history can indicate an episode of inciting trauma or the pain might just be insidious in onset. Local palpation can elicit tenderness. Rectal examination may be performed to palpate the coccyx between the forefinger and the thumb. This can help in eliciting any increased or decreased mobility of the sacrococcygeal segment by manipulation. Infection, masses and spasms of the muscles supporting the pelvic floor are to be ruled out. Dynamic X-ray imaging and MRI are helpful in detecting laxity, fractures, anatomical variations and other concomitant conditions like degenerative disc disease.
Treatment
Conservative treatment modalities usually are adequate in controlling the symptoms in majority of the patients.
Anti inflammatory medication may be initiated.

Heat & Cold Application In times of acute exacerbations of pain ,application of ice or a cold pack is recommended. In the period where the acute inflammation has settled local heat application can help in relaxing the spasming muscles.
Physical Therapy Pelvic floor rehabilitation exercises can help when muscles supporting the pelvic floor are the culprit. Manual massage and manipulation also are helpful in alleviating symptoms in some patients.
Lifestyle Modification This involves correcting the sitting posture and avoiding prolonged periods of sitting. Special U,V or wedge shaped pillows with a hole to accommodate the coccyx helps in relieving the pressure. These can be used while driving, at work or even on flights.
Nutritional Adjustment A high fibre diet with marked increase in water intake or even stool softeners might be ideal for people with tail bone pain associated with constipation.
AT ALLEVIATE
We follow a combination procedure of Ganglion Impar Injection,
Local trigger injection followed by local manual massage.
Ganglion Impar Injection
The ganglion impair is a terminal midline sympathetic ganglion which is present over the first coccygeal vertebral body and the sacrococcygeal junction. It is a very useful treatment modality as this block provides relief of coccydynia and pain involving the lower part of the rectum, anus, urethra, and vagina.
This procedure is performed with the patient in a prone position on the Operating table. Some practitioners like to prepare patients with laxatives the night before. With fluoroscopic guidance, a thin spinal needle is advanced through the sacrococcygeal hiatus. Needle placement is confirmed and dye spread is checked under fluoroscopy. Medication is delivered at the site of the Ganglion of Impar. This helps in blocking the sacrococcygeal plexus of nerves.
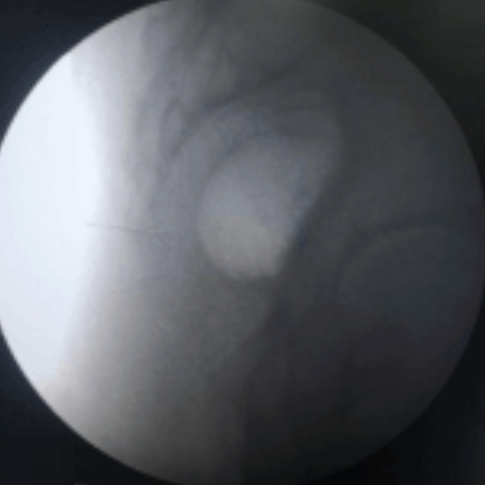
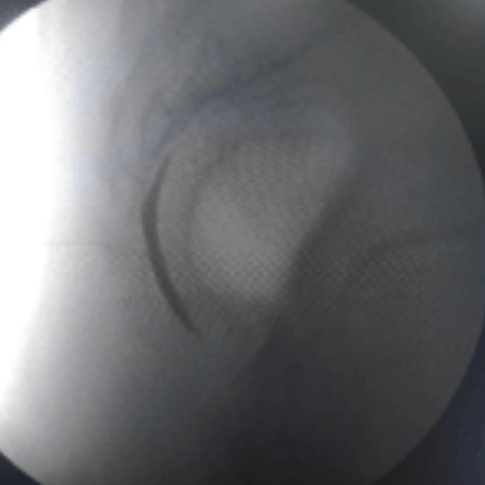
Lateral view
Intraop fluoroscopy image of ganglion impar injection
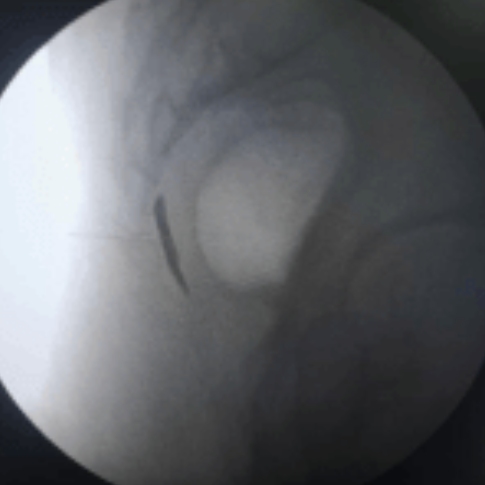
AP View
Intraop fluoroscopy image of ganglion impar injection
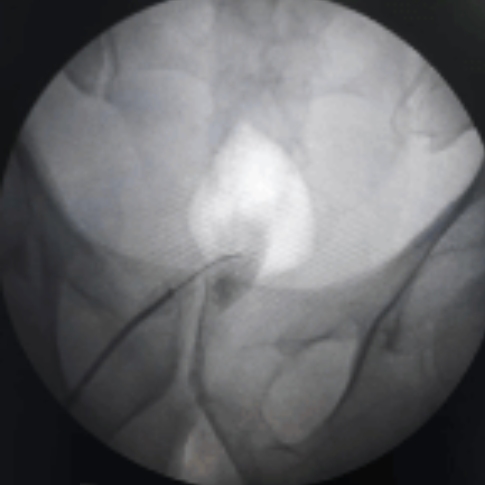
Intraop fluoroscopy image of contrast dye injection for confirmation of placement of needle
Intraop fluoroscopy image of contrast dye injection for confirmation of placement of needle
Intraop fluoroscopy video of contrast dye injection for confirmation of placement of needle
For chronic and resistant cases, the surgical approach is Coccygectomy. It is generally reserved as a last
resort owing to long and poor healing rates and high chances of post-operative infection.
FAQs - COCCYDYNIA/TAIL BONE PAIN
Coccydynia (Tailbone Pain) is a persisting pain felt at the very bottom of the spinal column in the region on the coccyx. The pain can be dull but aggravates sitting or while doing any activity. Patients can feel the pain to the distal most of the spine.
Tail bone pain called “coccydynia” is pain that occurs in and around the spine. The bone structure beneath the base of the spine (coccyx) – can cause pain due to falls, prolonged sitting position, or other factors like infection and tumors. Following are the causes of an event for tail bone hurt:
• External Trauma – A bruising, dislocation, or fracture of the coccyx.
• Internal Trauma – Trauma caused due to prolonged or obstructed labour, especially due to childbirth or from sitting on a narrow or hard surface for too long.
• Pregnancy/Childbirth
• Repetitive strain injury (RSI)
• Poor Sitting or Standing Posture
• Overweight or Underweight
• Cancer (rare case)
• Others – Degenerative disc disease, infections, abscesses, and tumors
• External Trauma – A bruising, dislocation, or fracture of the coccyx.
• Internal Trauma – Trauma caused due to prolonged or obstructed labour, especially due to childbirth or from sitting on a narrow or hard surface for too long.
• Pregnancy/Childbirth
• Repetitive strain injury (RSI)
• Poor Sitting or Standing Posture
• Overweight or Underweight
• Cancer (rare case)
• Others – Degenerative disc disease, infections, abscesses, and tumors
No. Tail bone pain is rarely lifelong.
Tail bone can last for days, weeks, months, or sometimes longer.
The symptoms of tailbone pain include:
• Pain due to dull, achy soreness, or piercing
• Pain aggravates due while sitting to standing up. Hard surfaces and unforgiving metal chairs can also annoy pain.
• Painful while getting up from sitting position or in some cases, a person can feel intense pain leaning for the support while standing or sitting.
• Pain during bowel movements
• Pain can occur during intercourse and defection
• Pain due to dull, achy soreness, or piercing
• Pain aggravates due while sitting to standing up. Hard surfaces and unforgiving metal chairs can also annoy pain.
• Painful while getting up from sitting position or in some cases, a person can feel intense pain leaning for the support while standing or sitting.
• Pain during bowel movements
• Pain can occur during intercourse and defection
You must immediately consult your doctor if you have pain in the tail bone and any other following symptoms:
• a sudden increase of pain or swelling
• constipation lasts long
• numbness, weakness, or tingling in one or both legs
• unable to perform bowels or bladder
• a sudden increase of pain or swelling
• constipation lasts long
• numbness, weakness, or tingling in one or both legs
• unable to perform bowels or bladder
Depending on your symptoms, your doctor will ask you to undergo a physical examination of the area. Rectal examination may also be performed.
Your doctor will ask to undergo tests – X-ray, Imaging, and MRI, which help in detecting laxity, fractures, anatomical variations, and other concomitant conditions like degenerative disc disease.
Your doctor will ask to undergo tests – X-ray, Imaging, and MRI, which help in detecting laxity, fractures, anatomical variations, and other concomitant conditions like degenerative disc disease.
Most of the tail bone pain is successfully treated using conservative treatment modalities. Based on the condition, anti-inflammatory medication is prescribed.
If there is an acute exacerbation of pain, ice or a cold pack is applied. Applying a local heat pack can help in relaxing the spasming muscles and relieves pain.
Under the physical therapist, pelvic floor rehabilitation exercises help in the complete relaxation of the muscles supporting the pelvic floor. Manual massage manipulation is helpful for muscles supported to the tail bone might help in relieving pain.
Your doctor may prescribe over-the-counter Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) to ease pain or discomfort until the tail bone heals. Drugs recommended by doctors are ibuprofen or naproxen, and Acetaminophen (Tylenol), also used to relieved tail bone pain.
Yes. Intake of fibre rich foods with a marked increase in water is good got tail bone. Stool softeners might help those associated with constipation.
Surgical procedure for tail bone is extremely rare as many patients have successfully treated with non-surgical techniques. During the surgery process, partial coccygectomy or total coccygectomy is surgically removed.
Although tail bone pain is uncomfortable it should not obstruct your daily activities. If you find any discomfort or difficulty, you need to contact your doctor immediately.
Most cases are cured by consulting with the pain management specialist doctor. However, booking an appointment with a highly experienced spine doctor helps in getting the best treatment.
Related Videos
Testimonials
References
[1]. Maigne JY, Doursounian L, Chatellier G. Causes and mechanisms of common coccydynia: role of body mass index and coccygeal trauma. Spine (Phila Pa 1976) 2000 Dec 1;25(23):3072–3079. [PubMed] [Google Scholar]
[2]. Maigne JY, Pigeau I, Aguer N, Doursounian L, Chatellier G. Chronic coccydynia in adolescents. A series of 53 patients. Eur J Phys Rehabil Med. 2011 Jun;47(2):245–251. [PubMed] [Google Scholar]
[3]. Schapiro S. Low back and rectal pain from an orthopedic and proctologic viewpoint; with a review of 180 cases. Am J Surg. 1950 Jan;79(1):117–128. [PubMed] [Google Scholar]
[4]. Nathan ST, Fisher BE, Roberts CS. Coccydynia: a review of pathoanatomy, aetiology, treatment and outcome. J Bone Joint Surg Br. 2010 Dec;92(12):1622–1627. [PubMed] [Google Scholar]
[5]. Pennekamp PH, Kraft CN, Stütz A, Wallny T, Schmitt O, Diedrich O. Coccygectomy for coccygodynia: does pathogenesis matter? J Trauma. 2005 Dec;59(6):1414–1419. [PubMed] [Google Scholar]
[6]. Thiele GH. Coccygodynia: Cause and treatment. Dis Colon Rectum. 1963 Nov-Dec;6:422–436. [PubMed] [Google Scholar]
[7]. Capar B, Akpinar N, Kutluay E, Müjde S, Turan A. Coccygectomy in patients with coccydynia [in Turkish] Acta Orthop Traumatol Turc. 2007 Aug-Oct;41(4):277–280. [PubMed] [Google Scholar]
[8]. Trollegaard AM, Aarby NS, Hellberg S. Coccygectomy: an effective treatment option for chronic coccydynia: retrospective results in 41 consecutive patients. J Bone Joint Surg Br. 2010 Feb;92(2):242–245. [PubMed] [Google Scholar]
© 2020-21 Alleviatepainclinic. All rights reserved.